Menstrual Leave in India
For Prelims: Article 21, Convention on the Elimination of All Forms of Discrimination against Women, Article 42, Rashtriya Kishore Swasthya Karyakram, SABLA programme
For Mains: Gender equality and labour rights in India, Menstrual health as a public health and social justice issue, Balancing workplace equality with gender-sensitive policies.
Why in News?
The Supreme Court of India (SC) expressed concerns that making paid menstrual pain leave a compulsory legal right could unintentionally harm women’s career prospects and employment opportunities, while hearing a petition seeking a uniform national policy on menstrual leave for working women and students.
- The petition argued that menstrual leave is part of the right to dignity under Article 21, and highlighted India’s commitment to the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW) and the absence of menstrual leave provisions in the Maternity Benefit Act, 1961.
Summary
- The Supreme Court of India expressed concerns that making paid menstrual leave a mandatory legal right could unintentionally lead to workplace discrimination and affect women’s career opportunities, while hearing a petition seeking a uniform national policy.
- The debate highlights the need to balance menstrual health, constitutional rights, and workplace equality, with the Court favouring voluntary policies and stakeholder consultation over a compulsory statutory mandate.
What are the Supreme Court’s Observations on Menstrual Leave Policies?
- Menstrual leave (or Period leave): It refers to workplace or academic policies allowing employees or students to take time off during menstruation due to pain or discomfort (dysmenorrhea).
- The leave may be paid, unpaid, or include rest breaks during the menstrual cycle.
- Medical studies suggest that over 50% of menstruating individuals experience menstrual pain for a few days every month.
- Around 15–25% experience moderate to severe pain, which can affect daily productivity.
- Supreme Court Observations: The Chief Justice of India noted that making menstrual leave a mandatory statutory right could lead to unintended workplace discrimination.
- The Court cautioned that mandatory menstrual leave may discourage employers from hiring women, as they may perceive them as a costlier workforce.
- The Court feared women might be denied leadership roles, promotions, or major responsibilities due to assumptions about frequent absences.
- The Court supported voluntary menstrual leave initiatives by states and companies, rather than a compulsory legal mandate.
- The Court stated that framing such a policy falls under the executive and legislature, advising the government to examine the issue after stakeholder consultation.
Judicial Pronouncements Regarding Menstruation
- Shailendra Mani Tripathi v. Union of India (2023): The Supreme Court declined to mandate a nationwide menstrual leave policy, citing complex policy implications, and advised the petitioner to approach the Ministry of Women and Child Development.
- The Court noted that while female labour force participation has risen significantly (23.3% in 2017-18 to 41.7% in 2023-24), many women, especially in informal and insecure employment, cannot afford to lose workdays, suggesting that support measures like free sanitary products and flexible leave provisions may be more practical.
- Dr Jaya Thakur v. Government of India & Ors. (2026): The Supreme Court of India recognised Menstrual Health and Hygiene (MHH) as a fundamental right under Article 21 (Right to Life and Dignity).
What are the Arguments in Favour of Menstrual Leave?
- Substantive Equality: Recognises that true workplace equality requires acknowledging biological realities such as menstrual pain (dysmenorrhea), which can affect productivity.
- Constitutional Basis: Menstrual leave can be justified under Article 21 (Right to Life and Dignity) and Article 42 of the Directive Principles of State Policy (DPSP), which call for humane working conditions and protection of health. Additionally, Article 15(3) empowers the State to make special provisions for women and children, providing a constitutional basis for such measures.
- Breaking Social Taboos: Formal recognition of menstrual leave can help destigmatise menstruation and normalise it as a natural biological process.
- Improved Health and Productivity: Allowing rest during severe menstrual pain can improve overall productivity and well-being by reducing stress and health complications.
- Gender-Sensitive Workplace Policies: Menstrual leave can make workplaces more inclusive and supportive for women, promoting gender-sensitive labour practices.
- Reduced Presenteeism: It helps address presenteeism (working while unwell), which often leads to lower efficiency and long-term health issues.
What is the Current Status of Menstrual Leave in India and Globally?
- No National Law: India currently does not have a central law mandating menstrual leave for women employees or students.
- State-Level Initiatives:
- Bihar allows two days of menstrual leave per month for women government employees (since 1992).
- Kerala provides menstrual leave and attendance relaxation for female students in universities.
- Private Sector Policies: Some companies such as Zomato, Swiggy, and Byju’s have introduced voluntary menstrual leave policies for their employees.
- Legislative Attempts: Private members’ bills such as the Menstruation Benefits Bill (2017) and the Right of Women to Menstrual Leave and Free Access to Menstrual Health Products Bill, 2022 have been proposed but none have been enacted into law.
- Global Practices: European nations like Spain and Sweden introduced state-funded paid period leave.
- Asian countries like Japan, South Korea, Vietnam, Philippines, Taiwan and Indonesia have menstrual leave laws.
- However, data shows that the actual utilization rate by women in these countries (especially Japan and South Korea) is extremely low, often under 1%, due to deep-seated cultural stigma and the fear of career repercussions.
Various Schemes to Promote Menstrual Hygiene Management
- The Right of Children to Free and Compulsory Education Act (RTE), 2009
- Menstrual hygiene scheme launched by the Ministry of Health and Family Welfare
- Rashtriya Kishore Swasthya Karyakram
- SABLA programme of Ministry of Women and Child Development
- National Rural Livelihood Mission of the Ministry of Rural Development
- Swachh Bharat Mission and Swachh Bharat: Swachh Vidyalaya (SB:SV)
- Guidelines for Gender Issues in Sanitation, 2017
- The National Guidelines on Menstrual Hygiene Management
- Scheme for Promotion of Menstrual Hygiene among adolescent girls in the age group of 10-19 years (supported by the National Health Mission)
What Measures can Strengthen Menstrual Health Support Without Undermining Workplace Equality?
- Adopt a “Health Leave” Framework: Introduce gender-neutral short-term health leave (2 days/month) applicable to conditions like severe migraines, dysmenorrhea, or endometriosis.
- This avoids hiring bias against women while still addressing menstrual health needs.
- Workplace Accommodation Model: Mandate reasonable workplace accommodations such as flexible hours, remote work, rest rooms, and lighter assignments during severe menstrual pain.
- Menstrual Health in Occupational Safety Standards: Integrate menstrual health into labour welfare and workplace health guidelines under labour codes and Occupational Safety, Health and Working Conditions Code, 2020.
- Evidence-Based Policy Making: Commission national studies on menstrual health, productivity loss, and workplace discrimination, enabling policy decisions grounded in data rather than assumptions.
- Targeted Support in Education Sector: Universities can adopt attendance relaxation policies and optional leave for students, similar to the Kerala model, to reduce dropouts linked to menstrual health issues.
- Corporate ESG Incentives: Encourage companies to adopt menstrual health policies as part of ESG (Environmental, Social, Governance) standards, linking gender-sensitive workplace practices with corporate ratings.
Conclusion
The menstrual leave debate underscores the need to balance women’s health and dignity with workplace equality. While the conversation on menstrual equity must continue, any policy should be legally anchored, socially sensitive, and practically enforceable, while remaining mindful of unintended consequences. Until then, “liberty to bleed” may remain more aspirational than real.
|
Drishti Mains Question: Discuss the constitutional and social dimensions of menstrual leave in India. Should it be a statutory right? |
Frequently Asked Questions (FAQs)
1. What is menstrual leave?
Menstrual leave refers to workplace or academic policies that allowwomen or menstruating individuals to take leave or rest during menstruation due to pain or discomfort (dysmenorrhea).
2. What is the current legal status of menstrual leave in India?
Indiadoes not have a national law mandating menstrual leave, though Bihar and Kerala have state-level provisions, and some companies offer voluntary policies.
3. Which constitutional provisions are linked to menstrual leave debates?
The issue is linked toArticle 21 (Right to Life and Dignity), Article 42 (humane working conditions), and Article 15(3) which allows special provisions for women.
4. What concerns did the Supreme Court raise regarding mandatory menstrual leave?
The Court warned that making menstrual leavecompulsory by law may discourage employers from hiring women and could negatively affect their career opportunities.
5. Which countries have menstrual leave policies?
Countries such asSpain, Japan, South Korea, Indonesia, Taiwan, Vietnam, and the Philippines have policies allowing menstrual leave, though usage rates remain low due to stigma and workplace concerns.
UPSC Civil Services Examination, Previous Year Question (PYQ)
Mains
Q. What are the continued challenges for women in India against time and space? (2019)
Q. Male membership needs to be encouraged in order to make women’s organisations free from gender bias. Comment. (2013)
Prison Health Crisis in India
Why in News?
The herpes simplex virus (HSV) outbreak in Jalpaiguri Central Correctional Home, has exposed the serious public health crisis in India’s prisons, driven by overcrowding, poor healthcare infrastructure, and staff shortages.
Herpes Simplex Virus (HSV)
- It is a common viral infection that causes painful blisters or ulcers and spreads through skin-to-skin contact with an infected person.
- It has two main types: HSV-1, which usually causes oral herpes (cold sores around the mouth), and HSV-2, which mainly causes genital herpes affecting the genital and surrounding areas.
- Many infected individuals show mild or no symptoms, though some may develop painful fluid-filled blisters, fever, body aches, and swollen lymph nodes.
- In rare cases, HSV can lead to serious complications such as meningitis or encephalitis.
- The infection remains in the body for life, but antiviral medicines can reduce symptoms and the frequency of outbreaks.
What are the Major Concerns Plaguing Indian Prisons?
- Overcrowding: According to the Prison Statistics India 2023 report released by the National Crime Records Bureau (NCRB), India’s prison occupancy rate stood at 120.8% in 2023, indicating persistent overcrowding.
- In several states, district jails record occupancy levels of 200–300%, leading to severe congestion and violations of inmates’ basic human rights.
- Several prisons in West Bengal exceed 160% occupancy, while Kandi Sub-Jail has historically crossed 400% overcrowding.
- A significant portion of the health crisis stems from the high number of undertrials, addressing this requires judicial intervention, expanded use of bail, and fast-tracking cases for minor offenses.
- Under Article 39A, free legal aid is a constitutional right, but the quality and accessibility of state-appointed lawyers remain poor.
- Many undertrials languish in jail simply because they cannot afford bail bonds or reliable legal representation.
- Prison Health Crisis: A 2023 study in The Lancet Public Health found prisoners in India five times more likely to develop tuberculosis (TB) than the general population.
- In Kerala prisons, about 30% of inmates were reported to have skin diseases due to humidity and overcrowding.
- The India Justice Report 2025 highlights that Human Immunodeficiency Virus (HIV) prevalence among prisoners is higher than the national average, linked to inadequate screening and shared equipment.
- Fungal infections (like ringworm) and scabies thrive in humid facilities where personal space and basic hygiene are severely compromised.
- Female inmates (who make up about 4% of the population) often lack access to gender-sensitive healthcare, basic hygiene products, and safe spaces for their children.
- Severe Mental Health Epidemic: The stress of incarceration, social isolation, and harsh environments lead to high rates of depression, anxiety, and Post-Traumatic Stress Disorder (PTSD).
- Some studies suggest that a vast majority of the prison population suffers from some form of mental illness or substance use disorder.
- In 2021, nearly four out of five “unnatural deaths” in Indian prisons were due to suicides, making suicide a leading cause of death among inmates, with rates significantly higher than in the general population.
- Human Resource Crunch: There is a 43% vacancy rate for medical officers, leading to an inmate-to-doctor ratio 2.6 times higher than the standards prescribed by the Model Prison Manual, 2016.
- India has only 25 psychologists for about 5.7 lakh inmates, reflecting a serious mental health care gap.
- Reactive, Not Preventive Care: Prison administrations often treat health issues reactively, waiting until an ailment is severe before providing care, rather than conducting regular preventive screenings.
How are Prisons Regulated in India?
- Constitutional Provisions:
- Article 21: Guarantees the right to life and dignity, protecting prisoners from torture and inhuman treatment and ensuring speedy trials.
- Article 22: Ensures that an arrested person is informed of the grounds of arrest and has the right to legal counsel.
- Article 39A: Provides free legal aid to ensure access to justice for the poor.
- Legal Framework:
- Model Prisons and Correctional Services Act, 2023: It replaces the colonial-era Prisons Act, 1894 and modernizes prison administration in India.
- Since prisons are a State subject, the Act serves as a model framework for States and Union Territories to adopt with necessary modifications.
- It also consolidates provisions from the Prisons Act, 1894, Prisoners Act, 1900, and Transfer of Prisoners Act, 1950.
- Model Prisons and Correctional Services Act, 2023: It replaces the colonial-era Prisons Act, 1894 and modernizes prison administration in India.
- Prison Reforms: The 2016 Model Prison Manual was introduced to standardise prison management, focusing on prisoner classification, medical care, and vocational training.
- In 2018, the Prisons Development Fund was launched to modernize prison infrastructure and support state-level improvements.
- International Frameworks: India follows global standards under Universal Declaration of Human Rights (UDHR) (1948), Declaration on Protection from Torture (1975), Convention Against Torture and Other Cruel, Inhuman, or Degrading Treatment (1984) on humane treatment of prisoners.
- Committees on Prison Reform:
- Justice Amitava Roy Committee (2018): Recommended establishing special fast-track courts to deal with petty offences and cases pending for over five years to reduce overcrowding.
- All India Jail Reforms Committee (1980-83): Emphasized that the prison system should be reformative, focusing on adequate food, clothing, sanitation, and the eventual rehabilitation of inmates.
- Justice V.R. Krishna Iyer Committee (1987): Focused on women prisoners, recommending exclusive institutions for women offenders staffed entirely by female personnel.
What Measures can Strengthen Prison Healthcare System?
- Adopt the Model Prisons Act, 2023: All States should adopt Model Prisons and Correctional Services Act, 2023, which includes provisions for gender-responsive healthcare, psychological counselling, and transfer of inmates with severe mental illness to specialised institutions.
- Ensure compliance with the Nelson Mandela Rules, 2015 (UN Standard Minimum Rules for the Treatment of Prisoners), guaranteeing healthcare standards comparable to the general population.
- Prison Decongestion: Strengthen Undertrial Review Committees (URCs) to identify prisoners eligible for bail or release, reducing overcrowding that fuels disease spread.
- Integrate Prison Healthcare with NHM: Link prison health services with the National Health Mission (NHM) and Ayushman Bharat for better staffing, medicines, and access to national disease-control programmes such as the National TB Elimination Programme.
- Conduct comprehensive medical screening at entry to detect infectious diseases like TB, HIV, and HSV.
- Telemedicine Facilities: Use platforms such as eSanjeevani integrated with the e-Prisons system to provide specialist consultations.
- Dedicated Psychiatric Services: Establish psychiatric wards and deploy clinical psychologists in prisons to address mental health issues and substance abuse.
- Specialised Care: Provide prenatal and postnatal care for women inmates, geriatric care for elderly prisoners, and safe facilities for transgender inmates.
- Improved Nutrition: Upgrade prison diets to address malnutrition and anemia, which increase vulnerability to infections.
- Alternative Sentencing: Under Bharatiya Nyaya Sanhita (BNS), 2023, expand the use of non-carceral punishments (like community service) and "open prisons" for non-violent, minor offenses.
Conclusion
Addressing poor prison healthcare infrastructure would help the State fulfil its constitutional obligation under Article 21 (Right to Life and Dignity), ensuring that loss of liberty does not mean loss of basic human rights and healthcare for prisoners.
|
Drishti Mains Question: Discuss the major health and human rights challenges faced by inmates in Indian prisons. How can prison reforms address these issues? |
Frequently Asked Questions (FAQs)
1. What is the Model Prisons and Correctional Services Act, 2023?
It is amodel legal framework issued by the Ministry of Home Affairs to modernise prison administration and replace the colonial-era Prisons Act, 1894, focusing on rehabilitation, healthcare, and prisoner welfare.
2. Why are Indian prisons considered a public health concern?
Overcrowding, poor sanitation, inadequate medical staff, and lack of preventive healthcaremake prisons vulnerable to outbreaks of diseases such as TB, HIV, and HSV.
3. What constitutional provisions protect prisoners’ rights in India?
Article 21guarantees the right to life and dignity, Article 22 ensures legal safeguards during arrest, and Article 39A mandates free legal aid for the poor.
4. What are the Nelson Mandela Rules?
TheUN Standard Minimum Rules for the Treatment of Prisoners (2015) set global standards ensuring humane treatment, healthcare access, and protection of prisoner rights.
5. Why is overcrowding a major issue in Indian prisons?
India’sprison occupancy rate exceeds 120%, largely due to the high number of undertrial prisoners, leading to poor living conditions, disease spread, and human rights violations.
National Vaccination Day and Universal Immunisation Programme
Why in News?
India celebrated National Vaccination Day (16th March) while highlighting major achievements of the Universal Immunisation Programme (UIP), including 98.4% full immunisation coverage by January 2026 and the launch of nationwide HPV vaccination and an indigenous Td vaccine in 2026.
National Vaccination Day
- National Vaccination Day is celebrated every year on 16th March to commemorate the first dose of Oral Polio Vaccine administered in India in 1995 under the Pulse Polio Programme.
- The programme led to the elimination of polio in India, with the last reported case in 2011 in Howrah, West Bengal.
What is the Universal Immunisation Programme (UIP)?
- About: The Universal Immunisation Programme (UIP) is a flagship public health programme of the Ministry of Health and Family Welfare aimed at providing free vaccination to children and pregnant women against vaccine-preventable diseases.
- It was originally launched as the Expanded Programme on Immunization (EPI) in 1978 and later expanded and renamed UIP in 1985.
- The UIP aims to increase immunisation coverage, improve the quality of vaccination services, establish a reliable cold-chain system up to health facilities, monitor programme performance, and achieve self-sufficiency in vaccine production.
- Integration with National Health Programmes: Over time, UIP has been integrated into several national health initiatives.
- It became part of the Child Survival and Safe Motherhood Programme in 1992, was included under the Reproductive and Child Health Programme in 1997, and since 2005 has been an integral component of the National Rural Health Mission (NRHM).
- Coverage and Scale: The UIP is one of the world's largest immunisation programmes, reaching 2.9 crore pregnant women and 2.54 crore newborns every year, free of cost.
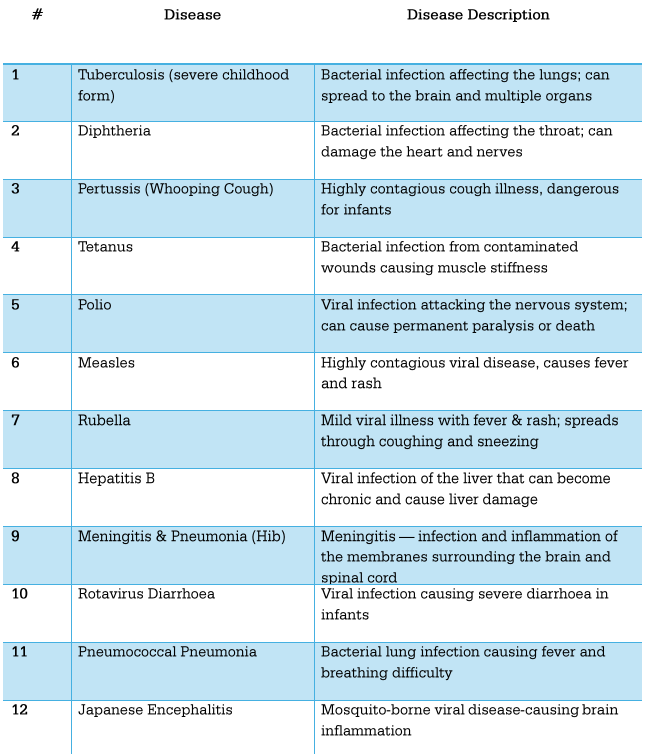
- Diseases Covered: Under UIP, free vaccines are provided to newborns, children, adolescents, and pregnant women against 12 vaccine-preventable diseases.
- While most vaccines are administered nationwide, the Japanese Encephalitis (JE) vaccine is provided only in endemic districts.
- Vaccines Introduced Under UIP:
- Inactivated Polio Vaccine (IPV) – 2015: Introduced as part of the Global Polio Endgame Strategy.
- Rotavirus Vaccine (RVV) – 2016: Introduced to reduce mortality from severe diarrhoea in children.
- Measles-Rubella (MR) Vaccine – 2017: Introduced through a nationwide campaign targeting about 41 crore children aged 9 months to 15 years.
- Pneumococcal Conjugate Vaccine (PCV) – 2017: Introduced to reduce infant mortality caused by pneumonia.
- Tetanus and Adult Diphtheria (Td) Vaccine: Replaced the TT vaccine to address waning immunity against diphtheria in adolescents and adults.
- Mission Indradhanush: Launched in December 2014, Mission Indradhanush aims to strengthen the UIP by increasing full immunisation coverage to over 90%, targeting unvaccinated and partially vaccinated children and pregnant women, especially in hard-to-reach areas.
- Launched in 2017, Intensified Mission Indradhanush (IMI) aims to vaccinate all children below two years and pregnant women left out of routine immunisation under the UIP, with a special focus on urban areas and low-coverage regions.
- Full immunisation coverage has risen from 62% in 2015 to 98.4% in January 2026.
- Infrastructure Supporting UIP Implementation:
- Vaccination Delivery Network: Under the UIP, vaccines are provided at Primary Health Centres (PHCs), Community Health Centres (CHCs), government hospitals, sub-centres, and outreach sessions at Anganwadi centres and village locations.
- Since 2005, UIP has been implemented under the National Rural Health Mission, including coverage in urban slums.
- Frontline health workers such as ASHAs (Accredited Social Health Activists), Anganwadi Workers (AWWs), and link workers play a crucial role in mobilising beneficiaries and ensuring that no child or pregnant woman is left unvaccinated.
- Model Immunisation Centres strengthen vaccination services. Such centres are already operational in Uttar Pradesh, Bihar, Chandigarh, and Ladakh.
- Cold Chain Infrastructure: Vaccines must be stored within a strict temperature range to maintain potency, which requires a robust cold chain system.
- India operates one of the largest vaccine cold-chain networks in the world, with over 1.06 lakh ice-lined refrigerators and deep freezers.
- This system supports over 1.3 crore immunisation sessions annually across the country.
- Digital Monitoring Systems: To strengthen vaccine logistics, the Electronic Vaccine Intelligence Network (eVIN) tracks vaccine stocks and storage temperatures in real time across the country, ensuring efficient supply chain management.
- U-WIN (2024) digital platform helps citizens locate vaccination centres, book appointments, and maintain vaccination records.
- CoWIN (2021), the digital platform used for Covid-19 vaccination registration and tracking, through which over 220 crore vaccine doses have been administered.
- Vaccination Delivery Network: Under the UIP, vaccines are provided at Primary Health Centres (PHCs), Community Health Centres (CHCs), government hospitals, sub-centres, and outreach sessions at Anganwadi centres and village locations.
What are the Milestones in India’s Vaccination Journey?
- Disease Eradication: India has successfully eradicated smallpox and eliminated polio (last case reported in 2011), yaws, and maternal and neonatal tetanus.
- Reaching the Unreached: The percentage of "zero-dose" children (infants who have not received any routine vaccinations) has been slashed by nearly half, dropping from 0.11% in 2023 to just 0.06% in 2024.
- Global Recognition: India's success in reducing child mortality and targeting leading infectious diseases has been explicitly recognized by the UN Inter-Agency Group for Child Mortality Estimation (2024), positioning the country as a global exemplar in child health.
- India’s Global Leadership in Vaccines and Pharmaceuticals: India ranks 3rd globally in pharmaceutical production by volume and exports medicines to around 200 countries, with the USA, Belgium, South Africa, the UK, and Brazil as major destinations.
- India produces about 60% of the world’s vaccines, making it the largest vaccine manufacturer globally, and supplies low-cost vaccines worldwide.
- The country is also the largest provider of generic medicines, accounting for around 20% of global supply by volume.
- During the Covid-19 pandemic, India supplied over 298 million vaccine doses to nearly 100 countries under the Vaccine Maitri initiative.
- To strengthen domestic pharmaceutical manufacturing and achieve self-reliance, the Government launched Production Linked Incentive (PLI) schemes for Bulk Drugs (2020), Medical Devices (2020), and Pharmaceuticals (2021) to boost investment and enhance global competitiveness.
Frequently Asked Questions (FAQs)
1. What is the Universal Immunisation Programme (UIP)?
UIP is aflagship vaccination programme launched in 1985 by the Ministry of Health and Family Welfare to provide free vaccines to children and pregnant women against 12 vaccine-preventable diseases.
2. What is National Vaccination Day and why is it celebrated?
National Vaccination Day is observed on 16 Marchto commemorate the first dose of Oral Polio Vaccine administered in 1995 under the Pulse Polio Programme, which helped eliminate polio in India.
3. What is Mission Indradhanush?
Launched in2014, Mission Indradhanush aims to increase full immunisation coverage to over 90% by targeting unvaccinated and partially vaccinated children and pregnant women, especially in hard-to-reach areas.
4. What is the role of eVIN in India’s immunisation system?
TheElectronic Vaccine Intelligence Network (eVIN) digitally tracks vaccine stock levels and cold-chain temperatures in real time, ensuring efficient vaccine logistics and supply management.
5. Why is India called the “Pharmacy of the World”?
India producesabout 60% of global vaccines and supplies around 20% of the world’s generic medicines, exporting pharmaceutical products to nearly 200 countries.
UPSC Previous Year Question (PYQ)
Prelims
Q. In the context of vaccines manufactured to prevent COVID-19 pandemic, consider the following statements: (2022)
- The Serum Institute of India produced COVID-19 vaccine named Covishield using mRNA platform.
- Sputnik V vaccine is manufactured using a vector-based platform.
- COVAXIN is an inactivated pathogen-based vaccine.
Which of the statements given above are correct?
(a) 1 and 2 only
(b) 2 and 3 only
(c) 1 and 3 only
(d) 1, 2 and 3
Ans: (b)
Q. With reference to recent developments regarding ‘Recombinant Vector Vaccines’, consider the following statements: (2021)
- Genetic engineering is applied in the development of these vaccines.
- Bacteria and viruses are used as vectors.
Which of the statements given above is/are correct?
(a) 1 only
(b) 2 only
(c) Both 1 and 2
(d) Neither 1 nor 2
Ans: (c)
Q. What is the importance of using Pneumococcal Conjugate Vaccines in India? (2020)
- These vaccines are effective against pneumonia as well as meningitis and sepsis.
- Dependence on antibiotics that are not effective against drug-resistant bacteria can be reduced.
- These vaccines have no side effects and cause no allergic reactions.
Select the correct answer using the code given below:
(a) 1 only
(b) 1 and 2 only
(c) 3 only
(d) 1, 2 and 3
Ans: (b)
Q. Which one of the following statements is not correct?(2019)
(a) Hepatitis B virus is transmitted much like HIV.
(b) Hepatitis B unlike Hepatitis C, does not have a vaccine.
(c) Globally, the number of people infected with Hepatitis B and C viruses arc several times more than those infected with HIV.
(d) Some of those infected with Hepatitis B and C viruses do not show the symptoms for many years.
Ans: (b)
Q. 'Mission Indradhanush' launched by the Government of India pertains to: (2016)
(a) Immunization of children and pregnant women
(b) Construction of smart cities across the country
(c) India's own search for Earth-like planets in outer space
(d) New Educational Policy
Ans: (a)
IPOs for Profitable RRBs
Why in News?
A Parliamentary panel has recommended launching Initial Public Offerings (IPOs) for highly profitable Regional Rural Banks (RRBs) to unlock their value, attract market capital, and enforce stronger corporate governance standards.
- An IPO is the process by which a privately held company offers its shares to the public for the first time, thereby transitioning into a publicly traded company. This enables the company to raise capital from a broad base of investors while allowing its shares to be listed and traded on a stock exchange.
What are the Key Observations of the Parliamentary Panel Regarding RRBs?
- Fiscal Performance: RRBs recorded a consolidated net profit of Rs 7,720 crore in the first nine months of FY 2025-26, bringing gross non-performing asset (GNPA) to a 13-year low of 5.4%.
- Successful Consolidation: Following the 4th phase of RRBs consolidation under the 'One State-One RRB' policy, the number of RRBs has been reduced from a peak of 196 to 28 in 2025-26 across 26 states and 2 UTs (Jammu & Kashmir and Puducherry).
- Sectoral Risks: Despite overall growth, priority sector education loans show a high GNPA of 13.8%. The panel suggests using AI-driven Early Warning Signals (EWS) and the Credit Guarantee Fund Scheme for Education Loans (CGFSEL) to mitigate this.
What are Regional Rural Banks?
- About: RRBs are specialised scheduled commercial banks established to provide accessible banking and credit services primarily in rural and semi-urban areas. They were designed to bridge the gap between the sophisticated commercial banking sector and the credit needs of the rural poor.
- Establishment and Legal Status: RRBs were created based on the recommendations of the Narasimham Working Group (1975). The first RRB, Prathama Bank, was set up on 2nd October, 1975. This was later formalized under the Regional Rural Banks Act, 1976.
- Purpose: To develop the rural economy by providing credit for agriculture, trade, commerce, and industry, particularly to small and marginal farmers, agricultural laborers, and artisans.
- Ownership Structure: Under the RRB Act, 1976 (amended in 2015), the current shareholding stands at Central Government (50%), Sponsor Banks (a Public Sector Bank, 35%), and State Governments (15%).
- Even after raising market capital, the combined shareholding of the Centre and Sponsor Banks cannot fall below 51%, ensuring continued public sector character.
- Key Characteristics and Operations:
- Area of Operation: Unlike Nationalized Banks, the area of operation for an RRB is limited to a specific region comprising one or more districts within a state.
- Priority Sector Lending (PSL): RRBs have a much higher mandate for rural credit. While commercial banks usually have a 40% Priority Sector Lending (PSL) target, RRBs must direct 75% of their total credit toward Priority Sectors (e.g., agriculture, MSMEs).
- Hybrid Nature: They combine the local feel and familiarity of cooperative banks with the professionalism and resource mobilization capacity of commercial banks.
- Regulation and Supervision: RRBs are regulated by the Reserve Bank of India (RBI) under the Banking Regulation Act, 1949, and must maintain a Capital to Risk-Weighted Assets Ratio (CRAR) of at least 9%.
- NABARD (National Bank for Agriculture and Rural Development) provides refinance facilities, conducts inspections, and supervises their performance.
- For taxation, they are treated as cooperative societies under the Income Tax Act, 1961.
What is the One State-One RRB Policy?
- About: The 'One State-One RRB' policy is a strategic initiative of the Department of Financial Services under the Ministry of Finance to consolidate multiple RRBs within a single state into a single, unified entity.
- Key Objectives: Key objectives include achieving economies of scale, eliminating redundancies from multiple administrative structures, rationalising costs, strengthening the capital base and financial resilience, and accelerating credit flow to priority sectors, particularly agriculture.
- Phase of Consolidation: The consolidation process began in 2005 based on the recommendations of earlier committees, notably the Vyas Committee (2001). Till early 2026, the government has carried out 4 phases of consolidatio
- Consolidations were executed under Section 23A of the RRB Act, 1976, through notifications issued by the Central Government.
Frequently Asked Questions (FAQs)
1. What are Regional Rural Banks (RRBs)?
RRBs are specialised scheduled commercial banks established under the Regional Rural Banks Act, 1976 to provide banking and credit services mainly in rural and semi-urban areas.
2. What is the ownership structure of RRBs?
As per the RRB Act (amended 2015), shareholding is Central Government (50%), Sponsor Bank (35%), and State Government (15%).
3. What is the ‘One State–One RRB’ policy?
It is a government consolidation initiative that merges multiple RRBs in a state into one unified bank to improve efficiency, capital strength, and credit delivery.
4. What is the Priority Sector Lending requirement for RRBs?
RRBs must allocate at least 75% of their total credit to Priority Sectors, significantly higher than the 40% target for commercial banks.
UPSC Civil Services Examination Previous Year Question (PYQ)
Q. Which of the following grants/grant direct credit assistance to rural households? (2013)
- Regional Rural Banks
- National Bank for Agriculture and Rural Development
- Land Development Banks
Select the correct answer using the codes given below:
(a) 1 and 2 only
(b) 2 only
(c) 1 and 3 only
(d) 1, 2 and 3
Ans: (c)
National Quantum Mission
Under the National Quantum Mission, 23 academic institutions have been approved to establish quantum teaching laboratories, with over 100 additional proposals currently under evaluation.
National Quantum Mission
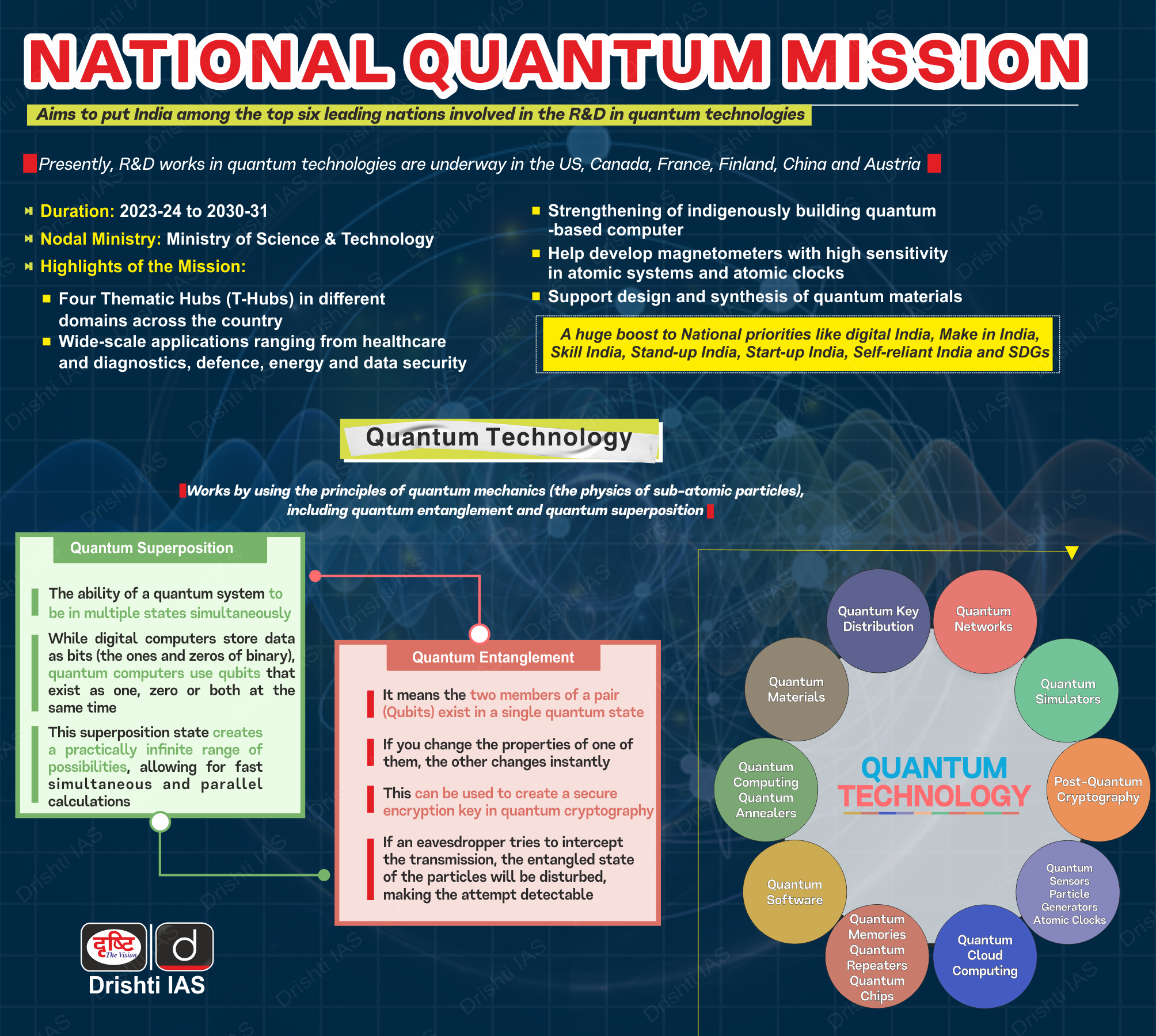
- About: NQM is a flagship initiative by the Department of Science and Technology (DST) with a total outlay of Rs 6,003 crore for the period from 2023-24 to 2030-31.
- It is designed to establish India as a leading global force in quantum technologies by fostering a vibrant ecosystem for scientific and industrial R&D.
- Objectives: The NQM aims to seed, nurture, and scale up R&D in quantum technologies to accelerate technology-led economic growth and build indigenous capabilities.
- Four Key Domains: The mission focuses on four main areas:
- Quantum Computing: Development of intermediate-scale quantum computers with 50 to 1,000 physical qubits within 8 years.
- Quantum Communication: Establishment of satellite-based secure communication over 2,000 km within India and long-distance inter-city Quantum Key Distribution (QKD).
- Quantum Sensing & Metrology: Creation of high-sensitivity magnetometers and precision atomic clocks for applications in navigation and communications.
- Quantum Materials & Devices: Advancement in fabrication capabilities for quantum materials to support indigenous hardware development.
- Implementation Structure (Hub-and-Spoke Model): The mission is executed through 4 Thematic Hubs hosted at premier institutions across India.
- Strategic Alignment: The NQM aligns with broader national initiatives like Digital India, Make in India, and Skill India, with a strong emphasis on strategic applications in security, defense, and critical infrastructure.
| Read More: National Quantum Mission |
Dual-Sex Crab of Silent Valley
Researchers have found a rare case of gynandromorphy—a condition where an organism displays both male and female characteristics (e.g., male reproductive structures alongside female gonopores)—in a freshwater crab species, Vela carli.
- Species & Location: Vela carli is an endemic freshwater crab species discovered within the tree holes of Silent Valley National Park in the Western Ghats.
- Scientific Significance: This study documents the first instance of gynandromorphy in the freshwater crab family Gecarcinucidae. While known in other crustaceans, it had never before been reported in this specific family.
- Crustaceans are aquatic invertebrate animals belonging to the arthropod group (animals with jointed legs and an external skeleton). It includes Crabs, Lobsters, Shrimp, Prawns, etc.
Silent Valley National Park
- About: Silent Valley National Park, located in the Nilgiri Hills of Kerala, is a pristine tropical evergreen forest. It is renowned as one of the last undisturbed tracts of the South Western Ghats and the core of the Nilgiri Biosphere Reserve (1986), India's first biosphere reserve.
- Geographical Feature: The Kunthipuzha River flows through the park. The name "Silent Valley" derives from the historical absence of noisy cicadas (sound-producing insects).
- Biodiversity Hotspot: It forms part of the Western Ghats World Heritage Site (UNESCO, 2012). The park is the most significant protected habitat for the endangered Lion-tailed Macaque, its flagship species. It also harbors the Nilgiri Langur, Malabar Giant Squirrel, Nilgiri Tahr, and great Indian hornbill.
- Historical Significance: In the 1970s, a proposed dam on the Kunthipuzha River sparked the "Save Silent Valley" movement (1973). It led to the project's abandonment and the area's declaration as a National Park in 1984.

| Read More: Western Ghats |
Reforms in India's Food Safety Framework
The Ministry of Health and Family Welfare (MoHFW) has approved a landmark set of regulatory reforms for the food sector, aligned with NITI Aayog's High-Level Committee on Non-Financial Regulatory Reforms, to balance Ease of Doing Business with robust food safety.
Reforms in India's Food Safety Framework
- Perpetual Validity of Licenses: The FSSAI has eliminated the requirement for periodic renewals; registrations and licenses will now have perpetual validity, significantly reducing compliance costs and paperwork for Food Business Operators (FBOs).
- The rationalization of licensing limits is designed to strengthen the role of State authorities, allowing them to focus resources on enforcement, monitoring, and capacity-building rather than routine renewals.
- Revised Turnover Thresholds: Effective 1st April, 2026, the turnover limit for registration increases from Rs 12 lakh to Rs 1.5 crore. State Licensing will now cover businesses up to Rs 50 crore, leaving Central Licensing for those exceeding this limit.
- Deemed Registration for Street Vendors: To remove dual compliance, street vendors registered under the Street Vendors (Protection of Livelihood and Regulation of Street Vending) Act, 2014, are now deemed registered under FSSAI, benefiting over 10 lakh vendors.
- For micro and small enterprises, these measures ensure instant registration, the elimination of pre-inspection, and a substantial reduction in interaction with licensing authorities.
- Risk-Based Inspection Framework: A new technology-enabled, dynamic risk-based inspection system has been introduced to prioritize oversight based on the nature of the food commodity and the past compliance record of the FBO.
Food Safety and Standards Authority of India (FSSAI)
- About: Established under the Food Safety and Standards Act, 2006, the FSSAI serves as the apex autonomous statutory body for consolidating food-related laws and ensuring public health through a single line of command.
- It operates under the Ministry of Health & Family Welfare (MoHFW), with a Chairperson holding the rank of Secretary to the Government of India.
- Regulatory Functions: It is empowered to frame regulations and standards for food products, grant licenses, and conduct scientific research and risk assessments on food safety.
- Key Campaigns: Major flagship programs include Eat Right India, State Food Safety Index, RUCO (Repurpose Used Cooking Oil), and the Food Safety Mitra scheme.
| Read More: FSSAI to Streamline Food Safety Regulations |
Sahitya Akademi Awards 2025
The Sahitya Akademi announced the Sahitya Akademi awards 2025 across 24 languages, honoring 8 poetry collections, 4 novels, 6 short story books, 2 essays, 1 literary criticism, 1 autobiography, and 2 memoirs.
- Notable winners include former diplomat Navtej Sarna for his English novel Crimson Spring, Hindi writer Mamta Kalia for her memoir Jeete Jee Allahabad and in the literary criticism genre, Tamil author Sa Tamilselvan for Thamiz Sirukathaiyin Thadangal.
- The award follows a July 2025 MoU between the Ministry of Culture and its 4 autonomous institutions—the National School of Drama, Sangeet Natak Akademi, Lalit Kala Akademi, and Sahitya Akademi—mandating a restructuring of awards in consultation with the Ministry.
Sahitya Akademi Awards
- About: The Sahitya Akademi Award, established in 1954, is the 2nd highest literary honor in India (after the Jnanpith Award) that recognises exceptional literary merit and promotes the country's rich multilingual heritage
- It is conferred annually by the Sahitya Akademi, an autonomous institution under the Ministry of Culture.
- Linguistic Coverage: The award is presented in 24 languages, which notably includes the 22 languages listed in the Eighth Schedule of the Constitution, plus English and Rajasthani.
- Eligibility: The work must be an original contribution published within the 5 years preceding the award year. The author must be an Indian citizen.
- Nature of the Award: One award is given per language each year for the most outstanding original book in recognized genres (such as poetry, novel, drama, or essays) published in the preceding five years.
- The recipient receives a copper plaque, a shawl, a citation, and a cash prize of Rs 1,00,000 (which has been steadily increased from its original value of Rs 5,000 in 1955).
- Other Notable Sahitya Akademi Honors: Yuva Puraskar (for young writers), Bal Sahitya Puraskar (for children's literature), Sahitya Akademi Fellowship, Bhasha Samman, etc.
| Read More: Sahitya Akademi Award 2024 |