SC Allows 1st Passive Euthanasia in Harish Rana Case | 13 Mar 2026
For Prelims: Supreme Court, Primary and Secondary Medical Boards, Bharatiya Nyaya Sanhita (BNS), 2023, Article 21 (Right to Life), Law Commission of India, High Court, National Health Mission 2013, Ayushman Bharat, National Programme for Non-Communicable Diseases 2010, National Programme for Health Care of the Elderly 2010, Pradhan Mantri Jan Arogya Yojana (PM-JAY), Ayushman Vay Vandana Scheme, Pradhan Mantri Ayushman Bharat Health Infrastructure Mission.
For Mains: Key observations of the Supreme Court in Harish Rana Case 2026, Key facts regarding Euthanasia, Key arguments for and against legalizing Euthanasia and way forward.
Why in News?
The Supreme Court (SC), in Harish Rana vs Union of India Case (2026), permitted passive euthanasia by allowing withdrawal of life support, marking the first application of the 2018 Common Cause judgment recognising the right to die with dignity.
Summary
- The Supreme Court of India allowed passive euthanasia for Harish Rana, a 32-year-old man in a permanent vegetative state for over 13 years, permitting withdrawal of life-sustaining treatment under medical supervision.
- The ruling applies earlier guidelines recognising the right to die with dignity under Article 21, marking India’s first court-approved implementation of passive euthanasia.
What are the Key Observations of the Supreme Court in Harish Rana Case 2026?
About the Case
- Harish Rana was a 19-year-old student in Chandigarh when he fell from a fourth-floor building in August 2013. The accident caused catastrophic brain injuries, leaving him in a Permanent Vegetative State (PVS) with 100% quadriplegia (paralysis of all four limbs).
- For nearly 13 years, he was sustained solely through Clinically Assisted Nutrition and Hydration (CANH) via surgically installed PEG tubes, with no sign of improvement. After the Delhi High Court dismissed his father's plea in 2024, the family approached the Supreme Court, which finally permitted passive euthanasia.
Key Observations of SC
- Acceptance of Medical Boards' Recommendations: The SC accepted the unanimous recommendation of medical boards and family members to withdraw life support and directed All India Institute of Medical Sciences, Delhi, to admit Harish Rana to its palliative care department and formulate a "robust, palliative, and end-of-life care plan."
- It emphasized that withdrawal must be carried out in a humane manner, managing pain and symptoms to ensure the patient's dignity is preserved and that it does not amount to "abandonment" of the patient.
- Status of Clinically Administered Nutrition (CAN): SC held that Clinically Administered Nutrition (CAN) administered through PEG (percutaneous endoscopic gastrostomy) tubes constitutes "medical treatment", not merely basic care.
- Therefore, its withdrawal falls within the scope of passive euthanasia and can be approved by the medical boards if it is not in the patient's best interest.
- Waiver of Reconsideration Period: To prevent unnecessary suffering, the SC waived the standard 30-day reconsideration period, allowing for the immediate implementation of the medical boards' decision to withdraw CAN.
Procedural Directives for Future Cases
To streamline the process nationwide, the SC issued specific directions:
- Streamlining Process: High Courts must instruct all Judicial Magistrates to receive and process hospital intimations regarding medical board decisions on passive euthanasia.
- The Union Government of India must ensure that Chief Medical Officers (CMOs) in all districts maintain a panel of Registered Medical Practitioners to serve on Secondary Medical Boards.
- Need for Comprehensive Legislation: The SC strongly urged the Union Government to enact a comprehensive law on end-of-life care. It warned that in the absence of such legislation, decisions are vulnerable to extraneous factors like financial distress, lack of insurance, or socio-economic vulnerability, which may impermissibly shape outcomes.
Living Will
- The SC defined a living will (advance medical directive) in the Common Cause v. Union of India (2018) as a written document that allows a patient to give explicit instructions in advance about the medical treatment to be administered when he or she is terminally ill or no longer able to express informed consent. It includes authorising their families to switch off life support in case a medical board declared that they were beyond medical help.
- The ruling significantly expanded patient autonomy by allowing individuals to retain control over end-of-life medical decisions even when they cannot communicate their wishes.
What is Euthanasia?
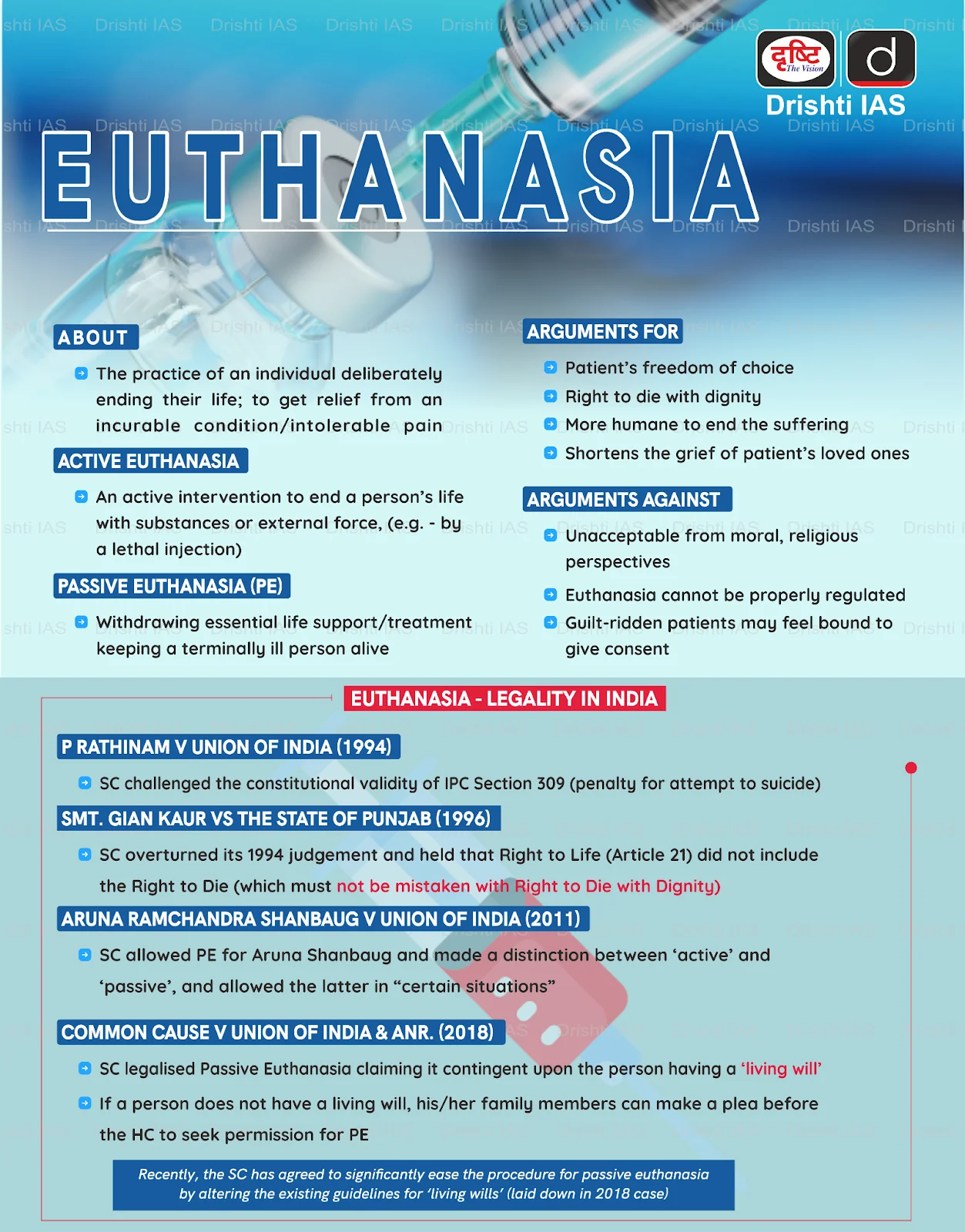
- About: Euthanasia is the deliberate, intentional act of ending a person's life in order to relieve them from persistent, unbearable suffering caused by an incurable or terminal illness, a condition of irreversible coma, or a persistent vegetative state.
- The term derives from Greek roots meaning "good death" (eu for good and thanatos for death) and is often framed as an act of mercy aimed at preserving dignity in the final stages of life.
- Classifications: It is primarily classified into two forms i.e., Active Euthanasia (a deliberate act, such as a lethal injection, to cause death) and Passive Euthanasia (withholding or withdrawing of life-sustaining medical treatment, allowing natural death to occur). These are further divided based on consent:
- Voluntary: Performed with the patient's explicit consent.
- Non-voluntary: Performed when the patient is incompetent to consent (e.g., coma).
- Involuntary: Performed without the patient's consent, which is widely illegal.
- Statutory Framework: Indian law draws a clear distinction between active and passive euthanasia.
- Active euthanasia remains explicitly prohibited under the Bharatiya Nyaya Sanhita (BNS), 2023, where intentionally causing death is treated as an offence under Section 100 (culpable homicide) or Section 101 (murder).
- However, the SC has legalized passive euthanasia in the Common Cause v. Union of India (2018) Case by recognizing the right to die with dignity as an integral part of Article 21 (Right to Life).
- The 241st Law Commission of India Report further clarified that a competent patient's refusal of life-sustaining treatment is legally valid, and doctors following such wishes cannot be charged with abetment or culpable homicide.
- Judgments Shaping Euthanasia in India:
- Maruti Shripati Dubal v. State of Maharashtra (1987): The Bombay High Court ruled that the right to die is inherent in Article 21 (Right to Life), permitting terminally ill patients or those in persistent severe pain to end their lives.
- Gian Kaur v. State of Punjab (1996): The SC reversed the above ruling and held that the right to life does not include the right to die, and emphasized the preservation of life.
- Aruna Shanbaug v. Union of India (2011): SC permitted passive euthanasia under strict legal and medical safeguards, even for patients unable to consent, marking a significant shift.
- Common Cause v. Union of India (2018): SC recognized the right to die with dignity, distinguished active euthanasia (not permitted) from passive euthanasia (permitted), and legally validated living wills (advance medical directives).
- Legal Process for Passive Euthanasia: The 2018 Common Cause guidelines, modified by the Supreme Court in 2023, establish a two-stage medical review process for passive euthanasia:
- Primary Medical Board: Formed by the hospital and consists of the treating physician and 2 independent doctors with at least 5 years of experience (reduced from 20 years).
- Secondary Medical Board: Comprises 3 independent doctors from a panel maintained by the District Medical Officer, who review the decision of the primary board.
- Both boards must provide their opinion, preferably within 48 hours, and their decision to withdraw treatment must be communicated to the Judicial Magistrate First Class (JMFC) along with the consent of the patient's family or guardian.
- Global Perspectives on Euthanasia: The legal status of euthanasia varies, with the Netherlands allowing both active euthanasia and assisted suicide; Switzerland permitting assisted suicide only, and Italy allowing passive euthanasia.
What are the Key Arguments For and Against Legalizing Euthanasia?
|
Category |
Arguments in Favor of Legalization |
Arguments Against Legalization |
|
Autonomy & Rights |
Individuals possess a fundamental right to self-determination, including control over their body and the timing/manner of death. Denying this infringes on personal liberty and dignity. |
There is no recognized "right to be killed"; the right to life (protected in constitutions and human rights frameworks) does not extend to a right to demand intentional termination by others. |
|
Compassion & Suffering |
In cases of terminal illness, euthanasia provides a merciful end, preventing prolonged agony and allowing a dignified death. |
Modern palliative care and pain management can effectively alleviate most suffering; euthanasia is unnecessary when high-quality end-of-life care is available and properly funded. |
|
Dignity & Quality of Life |
Prolonging life without meaningful quality can constitute cruelty; euthanasia permits controlled, peaceful exit rather than forced endurance. |
Human life holds intrinsic value regardless of perceived quality; legalizing euthanasia risks devaluing lives of the disabled, elderly, or chronically ill, implying some lives are "not worth living." |
|
Regulation & Safeguards |
With strict criteria (e.g., terminal illness, competent consent, multiple medical opinions), euthanasia can be safely regulated, as demonstrated in jurisdictions like India, the Netherlands, Belgium, and Canada. |
Experience in permissive jurisdictions shows a "slippery slope". Eligibility may extend beyond terminal cases to include non-terminal conditions, and mental illness, leading to involuntary or non-voluntary cases. |
|
Burden on Others |
Allows patients to avoid burdening family or society with prolonged care; reduces emotional and financial strain on loved ones. |
Legalization increases pressure on vulnerable individuals to choose death due to feelings of being a "burden" (e.g., rising percentages in Oregon,USA cite this factor), potentially masking coercion or inadequate support. |
|
Medical Profession |
Aligns with physicians' duty to relieve suffering; in hopeless cases, ending life compassionately fulfills a broader healing role. |
Contradicts core medical ethics (e.g., Hippocratic Oath: "do no harm") and the physician's role as healer/preserver of life; erodes patient trust and professional integrity. |
How can India Build a Better Support System for Terminally Ill Patients?
- Establish a National Palliative Care Mission: A dedicated National Palliative Care Mission, modelled on the National Health Mission 2013, should be launched to train healthcare workers and set up pain relief clinics.
- Ensure essential drugs like oral morphine (manage severe, chronic, or cancer-related pain) are available in every district.
- Integrated Public Health Systems: Palliative care must be integrated across all levels of healthcare—from Primary Health Centres (PHCs) to district hospitals—and coordinated with programmes such as Ayushman Bharat, the National Programme for Non-Communicable Diseases 2010, and the National Programme for Health Care of the Elderly 2010.
- Legal Literacy and Living Wills: Mass awareness campaigns must educate citizens about Advanced Directives (Living Wills). Hospitals should employ trained "patient advocates" to discuss end-of-life wishes with families.
- Strengthen Family and Community Support Systems: A comprehensive "Caregiver Support" model must provide respite care services, home care training, and psychological counselling for families.
- Community-based care should be revived by training local volunteers, replicating Kerala-based Neighbourhood Network in Palliative Care (providing home-based care for the chronically ill and dying).
- Ensure Financial Protection: Outpatient, home-based, and hospice palliative care must be fully incorporated into Pradhan Mantri Jan Arogya Yojana (PM-JAY) and the Ayushman Vay Vandana Scheme for senior citizens, covering essential medications, symptom management, and caregiver support to reduce catastrophic health expenditure.
- Leverage Technology: Tele-palliative care services should be expanded for rural areas using digital tools under Ayushman Arogya Mandirs. Robust monitoring mechanisms must track opioid availability and patient outcomes, supported by data from the Pradhan Mantri Ayushman Bharat Health Infrastructure Mission.
Conclusion
The Harish Rana case 2026 represents a compassionate evolution of Indian jurisprudence on end-of-life care. While legally permitting passive euthanasia under strict guidelines, the Supreme Court rightly emphasized building a palliative care support system. The path forward requires comprehensive legislation, streamlined procedures, and universal access to pain management to ensure dignity in death for all citizens.
|
Drishti Mains Question: Examine the legal and ethical dimensions of euthanasia. What are the arguments for and against its legalization? |
Frequently Asked Questions (FAQs)
1. What did the Supreme Court rule in the Harish Rana Case (2026)?
The Supreme Court permitted passive euthanasia by allowing withdrawal of Clinically Administered Nutrition (CAN) after approval by medical boards, reaffirming the right to die with dignity under Article 21.
2. What was the significance of the Common Cause v. Union of India (2018) judgment?
It legally recognized the right to die with dignity, validated living wills (advance medical directives), and established guidelines for passive euthanasia in India.
3. What is palliative care?
Palliative care is specialized medical care focused on relieving pain, symptoms, and stress of serious illness, aiming to improve quality of life for patients and their families.
UPSC Civil Services Examination, Previous Year Questions (PYQs)
Prelims
Q. Right to Privacy is protected as an intrinsic part of Right to Life and Personal Liberty. Which of the following in the Constitution of India correctly and appropriately imply the above statement? (2018)
(a) Article 14 and the provisions under the 42nd Amendment to the Constitution.
(b) Article 17 and the Directive Principles of State Policy in Part IV.
(c) Article 21 and the freedoms guaranteed in Part III.
(d) Article 24 and the provisions under the 44th Amendment to the Constitution.
Ans: (c)
Mains
Q. In order to enhance the prospects of social development, sound and adequate health care policies are needed particularly in the fields of geriatric and maternal health care.Discuss. (2020)